Juniper Publishers - Effectiveness of French Physiotherapy in Treating Congenital Clubfoot Deformity
Orthopedics and Rheumatology Open Access Journal

Abstract
Clubfoot is the most common congenital structural deformity that leads to physical impairments in children in many developing countries. Neglected clubfoot has been found to be a common cause of physical disability globally among children and young growing adults. The purpose of this study was to investigate the effectiveness of French physiotherapy in treating congenital clubfoot deformity. This cross sectional study was conducted among 102 parents and data were collected by face to face interview with semi-structured questionnaire. Statistical Package for Social Science (SPSS) was used to analyze the data. The mean age of the participants was 405 days. Unilateral limbs were more affected than bilateral limbs. Results shows that out of 30(100%) children with clubfoot deformity, 17(56.7%) were completed cured under French Physiotherapy while 8(26.7%) were completed cured under Ponseti method, almost equal number of children were in both group improved to moderate cured. There was significance difference found between two groups after intervention (p<0.05). French physiotherapy was more effective method for the treatment of clubfoot over the Ponseti method
Keywords: French Physiotherapy; Congenital Clubfoot
Introduction
Disability has emerged as a major public health problem worldwide. Childhood disability is one of them and it remains hidden in developing country like Bangladesh [1]. Importance of conservative treatment in congenital clubfoot has been known since the Hippocrates era (approximately 400 B.C) [2]. Continuous passive movement treatment method of French authors has also been added to manipulation, bandage, cast and device applications [3]. There is not a clear opinion in the literature on how to treat overcorrection. In the long-term follow-up studies, weakness in muscle groups around the ankle, joint stiffness was found [4,5]. Laaveg & Ponseti [6] obtained 89% success rate by using the conservative treatment method and minimal invasive surgery if required. Prevalence of congenital clubfoot in Bangladesh is high and most of the cases remain untreated or poorly treated [7]. According to French physiotherapy method (93-96%) so congenital clubfoot is manageable if the treatment can be started before child’s 1st birth day. It is important to identify the effectiveness of French physiotherapy in treating congenital clubfoot deformity than other conservative method like Ponseti Method. In French method the complication should be minimize. As there no study was done in this topic before in our country, I was very much interested to do research on this topic.
Material and Methods
Study design: Randomized clinical trial
Study population: Children with congenital clubfoot deformity who are attending the selective clinics.
Inclusion criteria:
- Willingly participating patients
- Age below 3 years
- Before tenotomy patients
Exclusion criteria:
- Benign feet
- Severe clubfoot deformity
- Before treated patient
Sampling technique
Treatment allocation: Treatment procedure was allocated randomly in two groups by tossing. The heads were taken in odd serial i.e. group -1 while the tails were placed in even serial i.e. group 2.
Group-1: This group was treated by Ponseti method [8-15].
Group-2: This group was treated by French physiotherapy methods. This treatment will carry out by a team with large experience in managing clubfoot with such a method [16,17]. In this study the sample size was taken as 30 for both group i.e Ponseti Method and French Physiotherapy Method.
Study place: The study was carried out at
- BCCW, Dhaka
- NGO- TLMB (Gaibandha), SEID Trust.
Study period and duration: From 14th January 2013 to 13th January 2014.
Data collection tool and instrument:
- Face to face interview of mother using pre-tested
structure questionnaire
- Face to face interview of mother using pre-tested
structure questionnaire
Data collection method
Data were gathered by pre verified semi structured questionnaires and in face to face interview. Information about pregnancy related question, family history & other characteristics was also obtained. The field work was conducted from March to September 2013 at Comilla & Dhaka district. The respondents were selected consecutively who will meet the inclusion and exclusion criteria. Two interviewers were trained for four days by the author. The training was consisted of lectures on how to fill up the questionnaires and mock interviews between participants.
Data analysis: Computer technology (SPSS 20.0) version was used for classification, presentation and analysis of data.
The Pirani score is a simple. The components are scored as follows:
- Each component may score 0, 0.5 or 1
- Hind foot contracture score (HCFS): Mid foot contracture score (MFCS):
- Posterior crease Medial crease
- Empty heel Curvature of lateral border
- Rigid equinus Position of head of talus (Table 1).
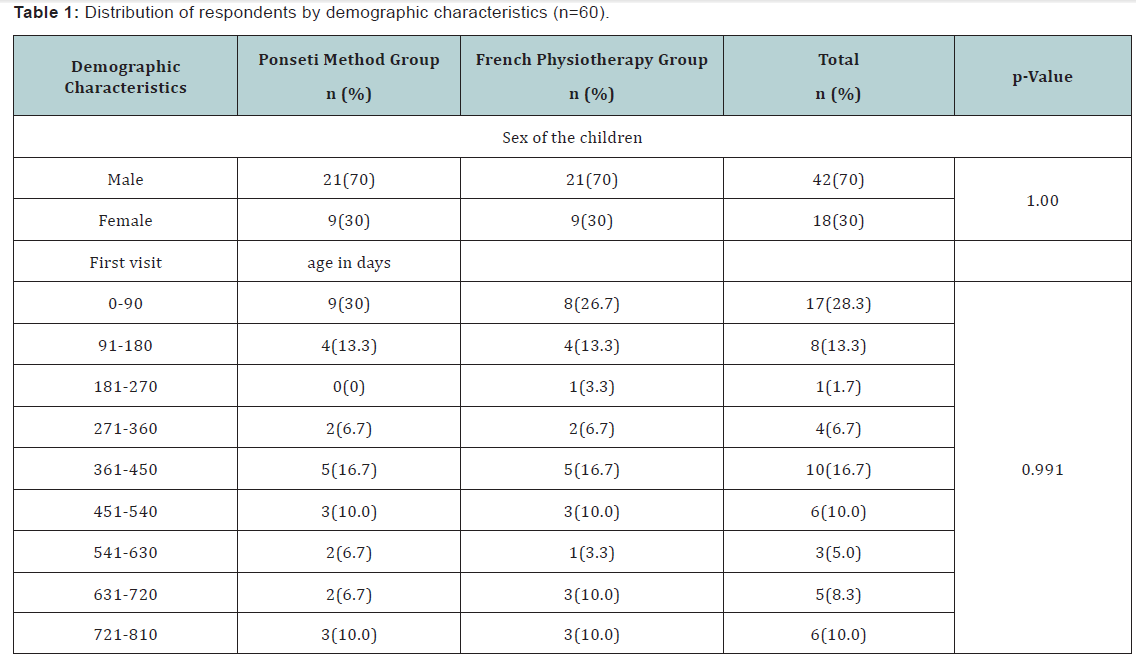
The mean age of the participants was 405 days, n=17 (28%) participants in between 0-90 days of age, n=8 (13%) in between 91-180 days of age and n=1 (2%) in between 181-270 days. n=4 (7%) participants in between 271-360 days of age, n=10 (17%) in between 361-450 days of age and n=6 (10%) in between 451- 540 days. n=3 (5%) participants in between 541-630 days of age, n=5 (8%) in between 631-720 days of age and n=6 (10%) in between 721-810 days. Result shows that 0-90 days are more common age those who had taken French physiotherapy & ponseti method. In control group the participants 21 out of 30(70%) were male and 9 out of 30 (30%) were female. Result shows that male was more affected than female. In intervention group the participants 21 out of 30(70%) were male and 9 out of 30 (30%) were female. Result shows that the male was more affected than female (Table 2).
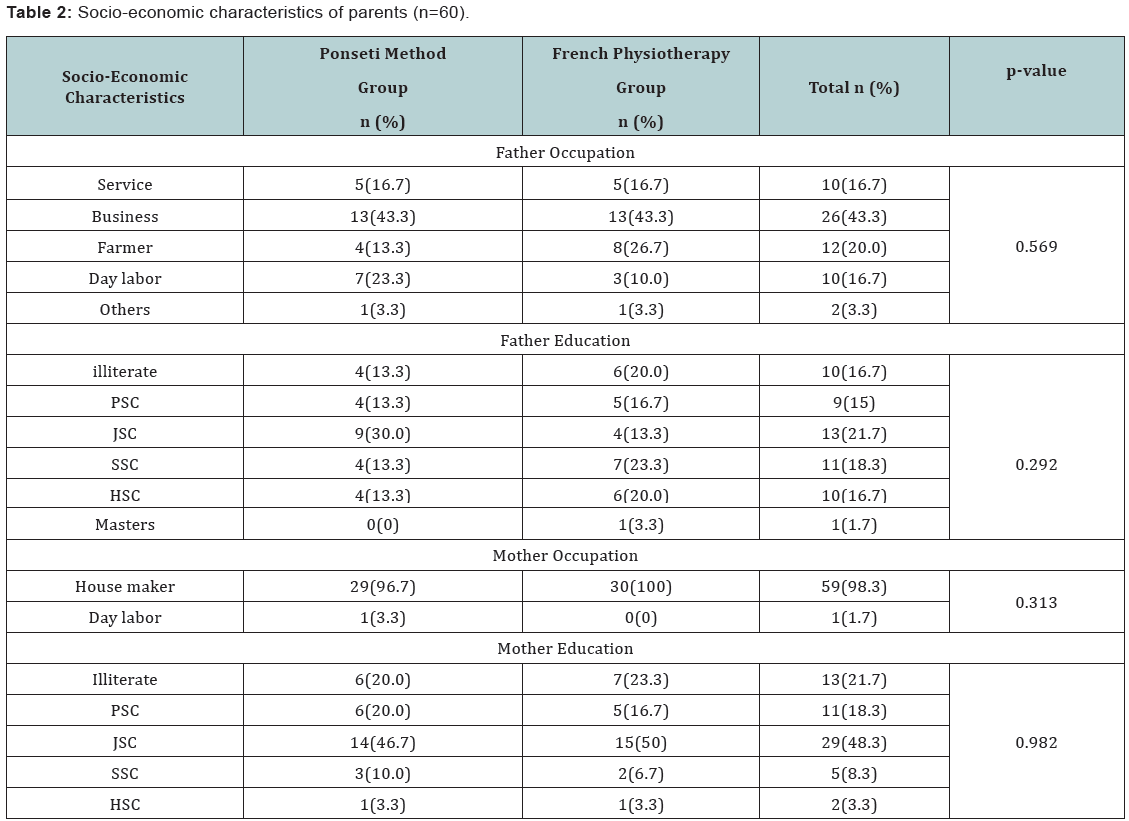
In terms of father occupation in ponseti group, out of 30(100%), 5(16.7%) were service holder while the equal number of service holders in French physiotherapy method group, 13(43.3%) were business holders in ponseti group while the equal proportion of respondents were business holders in French physiotherapy method group. Only 13% were farmers in ponseti group whereas the double proportion of fathers were farmers in France physiotherapy method group. Of the fathers in ponsity group 23% were day labor while the half of proportion were day labor in French group. In terms of father education almost equal proportion of fathers was same education level in both groups. Mother occupation indicates that almost all were house makers in both groups. Educational status was also same in both groups (Figure 1).
The above figure shows that almost equal proportion of father were same occupation in ponseti and French group. The majority were involved in business (Table 3).

Results
Result shows that among all the participants in Group A, unilateral n=47(78%) among them n=23(38%) were right limb affected & n=24(40%) were left limb affected and bilateral n=13(22%) were involvement of the affected limb of the participants. Result shows that unilateral limbs were more affected than bilateral limbs (Table 4).

Result shows that among all the participants approximately 5% (3 of 60) had past family history of clubfoot and 95% (57 of 60) had no past family history of club foot. Of them 2(6.7%) were in ponseti group and 1(3.3%) were in French Physiotherapy group (Table 5).
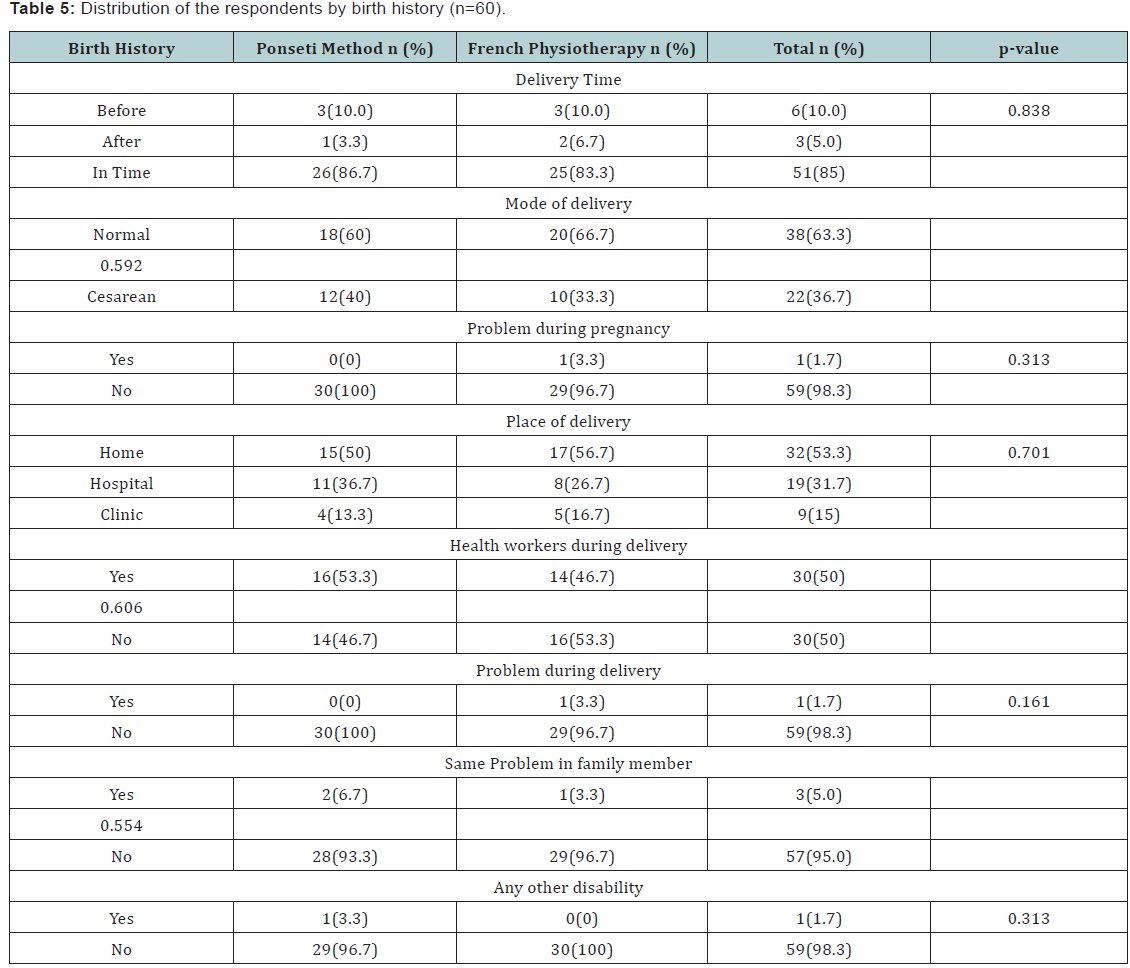
In both group 10% baby was preterm while 86% was born in time in ponseti group and 83.3% was in French group, the rest 3.3% in ponseti group and 5% was in France group was born in post term. Of the children with clubfoot deformity 60% had normal mode of delivery in ponseti group while 66.7% had in French group. Cesarean delivery had 40% in ponseti group and 33.3% had in French group. Problem during pregnancy occurred 0% in poseti group and 3.3% in French group. Place of delivery was home, hospital and clinic, the majority of the children’s place in delivery was home in both groups. It was about fifty percent. Only 13.3% had clinic in ponseti group and 16.7% in French group. Only 3.3% mothers had suffered problems during delivery while the rest had not suffered any problems during delivery. Of the mothers almost fifty percent had health workers during delivery, others had no health workers. Out of 30(100%) children, only 3.3% had other disability and it was in ponseti group (Table 6).

Results shows that out of 60(100%) children with clubfoot deformity equal numbers of them were in both group with severe and moderate deformity. There was no significance difference between two groups before intervention (p>0.05) (Table 7).

Results shows that out of 30(100%) children with clubfoot deformity, 17(56.7%) were completed cured under French Physiotherapy while 8(26.7%) were completed cured under Ponseti method, almost equal number of children were in both group improved to moderate cured. There was significance difference found between two groups after intervention (p<0.05). France physiotherapy was more effective method for the treatment of clubfoot over the Ponseti method (Table 8).

The above table shows that there was significance difference found between two methods in terms of clubfoot treatment (t=2.9, p=0.005). The calculated mean score was 1.1 and .53 in Ponseti and French physiotherapy method respectively. French Physiotherapy was more effective treatment for clubfoot deformity.
Discussion
The present study showed French physiotherapy was more effective method for the treatment of clubfoot over the Ponseti method. A study reporting early results of the Ponseti treatment, 95% of the deformities were corrected without need for extensive surgery [18]. This recovery rate is consistent with the results, reported by Herzenberg et al. [19], whose study included similar population and follow-up. Though it was not a new treatment method, Ponseti method had not been adopted by many and surgical treatment methods had been used as standard treatment until recent years. Initially, extensive surgical methods aimed physical improvement but owing to long term follow-up studies the importance of functional outcomes and maintenance of movement were recognized [20,21]. Muscular weakness and biomechanical changes [22-23], observed in patients who were considered as corrected initially, increased the popularity of conservative treatment methods again. Cooper & Dietz [24], found functionally and clinically perfect and good outcomes in 78% of deformities in patients, who were treated by Ponseti, in their average 30 years, follow-up study. This success rate was 85% in control group, consisting of the patients without congenital foot deformity. In their magnetic resonance imaging study, Pirani et al. [25] detected improvement in both the relation of tarsal bones and the forms of osteochondral outlines of the bones in patients, treated by Ponseti method. These findings support the Ponseti’s hypothesis, which asserts that with a proper treatment method that considers the functional anatomy of foot and uses biological potential in the tissues of a newborn, an appropriate improvement can be obtained in most of the deformities which is contradictory with the present study. The present study shows that there was significance difference found between two methods in terms of clubfoot treatment (t=2.9, p=0.005). Different conservative treatment methods have been suggested in the literature. One of the popular methods in Europe is the method of Dimeglio et al. [26] consisting of daily physiotherapy and continuous passive motion machine.
With this method, only 28% of the cases required surgical treatment. However, difficulties in long term physiotherapy, and its high cost makes adoption of this method problematic in many countries, including our country. In many countries, especially in the USA, Kite’s method has been used widely for a long time [27]. Kite, who tried to correct the components of the deformity separately and patiently, obtained improvement within 36 weeks. Ponseti attributes such a delay in improvement to the effort for correction of forefoot by counter pressure from calcaneocuboidal joint, which was Kite’s error according to Ponseti. Because kinematics of the foot does not allow evertion of calcaneus before abduction (outward rotation) of it, correction of varus became time consuming for Kite [28]. In a careful study, by Tümer et al. [29] where Kite’s and Ponseti’s manipulation methods were used concomitantly, it was reported that 33% of the cases were treated by only using plaster cast. This success rate reached at 41% with addition of the patients who underwent posterior release surgery. Bursalı [30] reported that they obtained correction in all of the untreated cases and in 75% of the cases, treated previously elsewhere, by using Ponseti’s method strictly.
Limitation
100% accuracy was not possible in any research so that some limitation may exist. Regarding this study, there were some limitations or barrier to consider the result of the study. The first limitation of this study was sample size. It was taken only 30 samples in each group. A very few researches have been done on a few of research among the effectiveness of French physiotherapy in management of clubfoot patients. So there was little evidence to support the result of this project study in the context of Bangladesh.
Conclusion
This study demonstrates that French physiotherapy method is an effective and reproducible method for correction of idiopathic Congenital Clubfoot deformities. Furthermore, it may be used in our country widely. For successful outcomes, this technique should be applied carefully and the patients should use the foot abduction orthosis with full compliance. For patient compliance, besides parent training, producing proper and comfortable shoes is required.
To Know More
About Orthopedics and
Rheumatology Open Access Journal Please click on:
https://juniperpublishers.com/oroaj/index.php
To Know More About
Open Access Journals Please click on:
https://juniperpublishers.com/index.php


Comments
Post a Comment