Evaluation of Cervical Capsular Ligament Injuries Following Whiplash Injury - Juniper Publishers
Orthopedics and Rheumatology - Juniper Publishers
Introduction
Traumatic sprain injury to the cervical spine is often much more serious than many clinicians suspect. Some patients may recover uneventfully from a spinal ligament sprain injury, but a significant number will have pain which may last indefinitely. This depends upon the Grade (degree of seriousness) of the spinal sprain that is present [1,2]. The risk of developing chronic pain will be increased if a clinician is unable to find a physical cause of pain in these patients. X-ray, CT, and MRI scan imaging techniques may not be able to show the real source of pain from injury, leading to a non-specific diagnosis and incomplete and or improper clinical treatment of the more serious grades of injury [2].
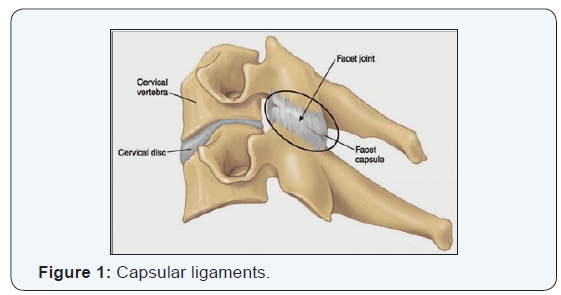
Capsular ligaments are the main stabilizer of the facet joints (Zygapophyseal joints) and have been implicated as a major source of chronic neck pain [3]. When injured they become elongated and exhibit laxity, causing excessive movement of cervical vertebrae [3]. After a spinal trauma, the spinal ligaments are often damaged causing abnormal motion due to ligamentous instability from the sprain (over-stretching or tearing) of the stabilizing ligaments. Yet, even serious intersegmental motion problems are routinely missed in standard X-ray and CT interpretations by qualified experts. One of the reasons is that some of the cervical spinal ligaments cannot be evaluated by standard X-ray views and other standard imaging protocols (Figures 1 & 2).

These facts are clinically significant. The cervical capsular ligament is the smallest, thinnest, most injured ligament in a spinal trauma. It is also the least assessed ligament in a spinal trauma. This seems to make no sense, but the fact is, none of the standard imaging views of any standard protocol, assess this ligament properly. Special views are needed. That will be the focus of this survey, as most clinicians from multi-disciplinary health fields agree that these are serious injuries, and yet are commonly miss-diagnosed or not diagnosed at all. In preparation of this article multiple peer-reviewed published research articles were reviewed, all agreeing that chronic pain from spinal joint instability is a very significant clinical problem, causing significant clinical symptoms of chronic pain indefinitely, and may be the number one cause of chronic pain on the globe; yet few if any of those same published articles were in agreement as to a standard, objective diagnostic work-up, and/or treatment of the problem itself.
Note for Reference
“There has yet to be a standardized functional x-ray able to diagnose cervical instability or detect ruptured ligamentous tissue without the presence of bony lesions [3]. In one autopsy study of the cervical spine, only one out of 10 gross ligament disruptions was evident on standard x-rays. Even after severe whiplash, plain radiographs are usually normal despite clinical findings indicating the presence of soft tissue damage [4]. Imaging scans like certain specialty MRI, fCT, and DMX may be able to depict cervical instability pathology, [5,6] but may not quantify it for severity. The focus of this current survey is to reveal the commonality of cervical capsular spinal ligament injury and the “miss-rate” of diagnosing cervical capsular spinal ligaments for injury, as well as indicating a standard, accurate, and efficient way to make this necessary evaluation.
Case Selection
For this survey, 105 consecutive cases of diagnosed whiplash sprain injury as a result of motor vehicle trauma were reviewed. Each case was assessed for spinal ligament instability as a standard protocol, using accepted computerized radiographic mensuration analysis (CRMA), which is the most accurate method available to measure and assess translation and angular abnormalities according to the standards of the AMA Guidelines to the Evaluation of Permanent Impairment, (5th Edition) and December 15, 2000 [7]. This method of quantification is determined to be more accurate by far, than the next best available methods, for evaluation of standard diagnostic spinal x-rays. However, note that most standard diagnostic spinal x-rays do not typically include views that would accurately assess capsular ligaments of the facet joints.
In each case, there happened to be at least one vertebral level that was measured for spinal ligament injury of some Grade, ranging from mild to very severe (Grades II, III, or IV), based upon accepted Arthur Croft Guidelines for the evaluation of Cervical Whiplash Injury, that are incorporated into the National Guidelines Clearing House [8]. None of these grades of injury were reported on the initial pathology read from the radiologist, and all would potentially have been missed without accurate measurement by Computerized Radiographic Measurement Analysis (CRMA) [9].
Demographics
All 105 cases revealed a degree of ligament injury at 1 or more level(s). There were 77 spinal levels revealed to have measurable abnormal angular findings. There were 359 spinal levels revealed to have measurable Translation findings. This is a total of 436 individual levels of spinal ligament injury.
There were 26 angular measurements that revealed permanent cervical spine ligament injury according to AMA Guidelines for measurement, 28.6% (Grade III-IV Sprain injury).
There were 56 angular measurements that revealed permanent cervical spine ligament injury according to AMA Guidelines for measurement, 15.6% (Grade III-IV Sprain injury). These documented clinical findings show that the CRMA (Computerized Radiographic measurement Analysis) is without doubt a premier diagnostic screening tool for accurately evaluation spinal ligament injury. Of specific interest for this study, there was no direct mention of capsular ligament injury for any patient’s case, in the official documentation of the Radiologists standard pathology report on diagnostic spinal x-rays.
Additional specialty testing revealed 93 of these same 105 patients, 88.6%, did have capsular ligament injury to some degree. The various treating doctors “suspected” ligament injury in general from their clinical indications on examination, but none of them specifically mentioned capsular ligament injury, so 100% of the 93 patients who had capsular ligament injury may have not had it diagnosed, if they used only standard diagnostics. These same cases were also assessed by Digital Motion X-Ray (DMX). Digital motion X-Ray is a modern up-dated version of fluoroscopy, also sometimes call cineradiography, using computer enhancement which results in a much clearer image, while using approximately 1% of the radiation exposure of traditional Fluoroscopy. The pulsed X-Ray system with computer enhancement allows for exposure at 3MA, as opposed to the standard 300 MA of regular Diagnostic X-Rays. It should in no way be confused with traditional fluoroscopy or cineradiography. Full motion of the cervical spine is captured in real time and recorded as a motion picture on DVD.
Part of the 8 view assessment protocol of DMX is to view spinal motion in the position of oblique flexion. No other standard X-ray procedure requires this view, but it is the only view that allows for specific and accurate assessment of the facet joint motion and cervical capsular ligament. The results of the Board Certified Medical Radiologists performing this DMX assessment revealed that 93 of these same 105 patients, 88.6%, did have capsular ligament injury to some degree. The Radiologist’s assessments also revealed that 52 of these patients had multiple levels of capsular ligament injury in the cervical spine (Figure 3).
Summary
In Summary there were a total of 436 individual levels of spinal ligament injuries measured by computer mensuration on 105 patients that were not revealed on standard pathology reads.
There were an additional 243 levels of separate spinal capsular ligament injuries revealed by Digital Motion X-Ray that were not revealed by the Radiologist pathology report. This is interpreted that 55.73% of significant clinical injuries were missed by standard imaging evaluations alone (Table 1). There was an 88.5% correlation of capsular ligament injury when accurate measurement revealed angular findings on standard x-rays (23 out of 26).
Conclusion
- Capsular ligaments are the main stabilizer of the facet joints and have been implicated as a major source of chronic neck pain.
- When injured they become elongated and exhibit laxity, causing excessive movement of cervical vertebrae. Serious intersegmental motion problems are routinely missed in standard X-ray and CT interpretations even by qualified experts.
- Computerized Radiographic Measurement Analysis (CRMA) is a valuable and essential tool in the initial assessment of standard x-rays of patients in a trauma, noting that the AMA Guidelines and others require accurate assessment of stress-radiographs after suspected cervical spine injury.
- Cervical capsular ligament is the smallest, thinnest, most injured ligament in a spinal trauma. It is also the least assessed ligament in a spinal trauma, using standard protocols for imaging.
- When Angular findings are accurately measured as determined by CRMA and found to be serious ratable severe sprain injuries, 88.5% of these patients had significant capsular ligament injury as well, which would have been missed on standard radiology reads, making accurate assessment of capsular ligaments essential.
- Under-utilized, Digital Motion X-Ray (DMX) is an accurate diagnostic modality that can detect spinal capsular ligament injury, especially given the fact that standard Diagnostic spinal x-rays do not include views to make this specific assessment. Given the seriousness of spinal capsular ligament injury, and given the commonality of occurrence that this survey and other studies, have revealed, one can conclude that the Digital Motion X-Ray assessment should be considered whenever capsular spinal ligament injury is clinically indicated. (It may be indicated when clinical cervical spine symptoms persist 8-12 weeks after initial treatment, according to some published Professional Guidelines) [10-13].
- There is direct clinical application for doctors who treat spinal injury from trauma, from conservative treatment like Chiropractic care, Medical pain management specialists who perform facet injections, to Surgeons who perform spinal fusion surgery and or new prolotherapy options which can now stabilize unstable joints once properly diagnosed, by actually repairing the torn ligament.
Regardless of various treatment options among specialty physicians, detection and diagnostic assessment remains the key for any and all clinicians. CRMA and Digital Motion X-ray are both invaluable tools that should be incorporated into cervical spine ligamentous assessment after trauma.
To Know More About
Orthopedics and Rheumatology Open Access Journal Please click on:
https://juniperpublishers.com/oroaj/index.php
For more Open
Access Journals in Juniper Publishers please click on:
https://juniperpublishers.com/index.php
For more about Juniper Publishers Please click on:
https://juniperpublishers0.wixsite.com/juniperpublishers


Comments
Post a Comment